- Visibility 293 Views
- Downloads 48 Downloads
- Permissions
- DOI 10.18231/j.ijpca.2024.003
-
CrossMark

Therapeutic landscape of natural products and emulgel in psoriasis
- Author Details:
-
Ritik Matade
-
Swarup Harne
-
Sakshi Kale
-
Yashodhan Ponde
-
Tejas Naik
-
Ganesh Lamkhade
-
 Rohit Doke *
Rohit Doke *
Abstract
Psoriasis, characterized by immune-mediated inflammation triggered by dysfunctions in the immune system, manifests in various skin areas with elevated plaques presenting as common symptoms. Traditional psoriasis treatments often incorporate plant-based remedies, which, although safer, are predominantly hydrophobic, limiting their permeation and absorption into the skin. To address these challenges, researchers have turned to emulgels as drug delivery systems. Emulgels, combining the properties of both emulsions and gels, effectively solubilize hydrophobic drug molecules, enhancing their absorption through the skin. Emulgels shows several advantages including easy application and removal, emollient properties, non-greasiness, cosmetic appeal, and excellent penetration capabilities.
This review emphasizes the significance of herbal drugs in psoriasis therapeutics and explores the utilization of emulgels as a delivery system for herbal extracts and constituents in psoriasis treatment. By highlighting the potential of emulgels in enhancing the delivery of herbal remedies for psoriasis management, this review offers insights into novel approaches to address the challenges associated with traditional psoriasis treatments.
Introduction
Psoriasis is a multifaceted condition affecting approximately 2% of the global population, with higher prevalence observed in Caucasian, Asian, and Black demographics. It exhibits geographical variation, being more common in colder northern regions and less prevalent in tropical climates in Europe.[1] The disease can manifest at any age and is characterized by intricate pathophysiological mechanisms. Psoriasis, an enduring autoimmune skin disorder, has been recognized since ancient times and is typified by the gradual enlargement and shedding of psoriatic plaques alongside pustules and spots, originating in the papillary dermis. Anomalies in keratinocyte proliferation and migration result in epidermal thickening, incomplete differentiation, and parakeratosis. [2] As the condition progresses, certain skin cell populations excessively proliferate, leading to acanthosis nigricans. Typically, psoriasis presents as red, inflamed patches with silvery-white scales, often symmetrically distributed. It is classified as an autoimmune ailment and is associated with immune system dysfunctions involving T cells, dendritic cells, and cytokines like interleukin 23, interleukin-17, and tumor necrosis factor. Psoriasis stands as the most common genetic skin disorder and correlates with heightened risks of metabolic syndrome and cardiovascular disease. Severe forms of psoriasis are linked with components of metabolic syndrome, including obesity, dyslipidemia, diabetes mellitus, and hypertension. [3] Despite conventional therapies providing symptomatic relief, a definitive cure remains elusive, with many treatments carrying adverse effects such as atrophy, organ toxicity, immunosuppression, infection, and carcinogenesis.[4]
Recent years have witnessed growing interest in drug carriers, offering solutions to various diseases by addressing issues such as low bioavailability, poor solubility in water, and biological degradation of medicinal substances. Topical drug delivery systems are frequently employed for localized effects on the skin, catering to cosmetic and dermatological needs, including the treatment of skin disorders like eczema, acne, and psoriasis. [5] These systems, however, can also exert systemic effects through transdermal delivery, enhancing patient compliance and facilitating self-medication. Hydrogels emerge as modern and versatile drug delivery vehicles owing to their highly adjustable physical properties. [6] Comprising primarily water and a polymer forming a three-dimensional network structure through chain cross-linking, hydrogels exhibit porosity, accommodating drug molecules. Nonetheless, a notable drawback of hydrogels is their inability to deliver hydrophobic drugs, a major challenge given the hydrophobic nature of many effective drug substances. To overcome this limitation, emulgels, also known as creamed gels and gelled emulsions, have been developed. Emulgels represent innovative drug delivery systems formed by blending emulsions and gels, possessing characteristics of both while offering dual-controlled release capabilities, alongside numerous desirable attributes and high patient acceptability. [7]
In recent years, emulgels have emerged as promising delivery platforms for both hydrophilic and lipophilic functional compounds and nutraceuticals, including carotenoids, vitamins, probiotics, and unsaturated fatty acids. These systems offer solutions to challenges such as low chemical stability, limited solubility, and poor absorption of food ingredients, while also enhancing the sensory qualities of formulations, bioavailability, bio-accessibility, and controlling their release. [8], [9] Researchers have shown particular interest in protein-based emulsions derived from sources like casein, soy, gelatin, and whey protein due to their effective emulsifying and gelling properties, as well as their abundance and renewable potential. Emulgels designed for food applications offer advantages over traditional emulsions, including slower release of active compounds in the intestines due to improved stability in gastric and intestinal environments. This enhanced stability is attributed to structural changes in emulsion gels during digestion, which inhibit the action of lipases on oil droplet surfaces, thereby reducing lipid digestion and the release of incorporated ingredients. [10] Through careful selection of emulgel excipients, desired release profiles can be achieved in a controlled manner. Moreover, ongoing research explores the development of emulgels as stimuli-responsive systems, capable of altering their morphology and properties in response to external stimuli. [11]
The article presents scientific findings supporting the efficacy of natural substances in the treatment of Psoriasis. It comprehensively examines in vitro, in vivo, and clinical studies investigating plant-derived compounds and their effects on psoriatic symptoms, immunomodulation, and anti-inflammatory responses. Providing detailed insights into psoriasis pathogenesis, inflammation, oxidative stress, and molecular interactions between natural compounds and the immune system, the article aims to enhance understanding of their therapeutic potential. Moreover, the review explores the utilization of natural products and emulgels as potential treatments for psoriasis. It delves into their effectiveness, mechanisms of action, and clinical applications in managing psoriasis, focusing on their therapeutic benefits and potential impact on the treatment landscape for this skin condition. By synthesizing evidence from various studies, the article seeks to shed light on the role of natural substances and emulgels in psoriasis management, offering valuable insights for researchers and clinicians alike.
Pathogenesis of Psoriasis
Psoriasis's origins are intricate, stemming from an abnormal immune response in the skin influenced by both genetic factors and environmental triggers. Treatment primarily focuses on addressing autoimmune-related mechanisms involving immune system cells and cytokines. The skin's microbiota contributes to immune system regulation, while genetic predispositions are significant contributors to psoriasis inheritance. Mutations in regulatory proteins within immune cells result in altered cytokine expression, impacting the proliferation and differentiation of keratinocytes. Variants of immune cells and proteins linked to psoriasis contribute to varying disease courses. Epigenetic modifications, including DNA methylation, histone modifications, and non-coding RNAs, represent a recent addition to our understanding of psoriasis pathophysiology. [12], [13], [14]
Immune system dysfunction and psoriasis
A defining trait of psoriasis is persistent inflammation, which triggers the excessive proliferation and irregular differentiation of keratinocytes. Histologically, psoriatic plaques exhibit epidermal hyperplasia, accompanied by inflammation comprising dermal dendritic cells, macrophages, T cells, and neutrophils. In psoriatic alterations, two distinct sets of cellular responses disrupt the equilibrium between innate and adaptive immune cell activation and the factors secreted by keratinocytes, consequently impacting T cells and dendritic cells directly.
Key players in congenital immunity during psoriatic changes include neutrophils, plasmacytoid dendritic cells (pDCs), and CD11c+ dendritic cells. Neutrophils undergo continuous production in the bone marrow and subsequent transportation to the bloodstream. Chemokines such as interleukin-8 (IL-8), CXCL1, and proteins like S100A7/A8/A9, released by keratinocytes, establish a chemotactic gradient facilitating neutrophil migration to the epidermis. PDCs, characterized by BDCA-2+ and CD123+ antigen expression, are known for their high production of interferon-α (IFN-α) upon activation, and are thought to play a pivotal role in initiating disease-related changes.
The presence of abundant T cells and mature dendritic cells (DCs) in skin aggregates, along with the expression of lymphoid-attracting chemokines such as CCL19, CCL21, CXCL12, and CCL18, may facilitate the activation of T cells within the skin itself. T cells in psoriatic alterations are classified into two functional groups: helper T cells (TH) and cytotoxic T cells (TC). A subset of T cells expresses CD161 and other cytotoxic receptors, indicating the involvement of natural killer T cells in psoriasis pathogenesis. Cytokine interactions in psoriasis are thought to follow a model where inducers such as IL-23 or IL-12 trigger the production of IFN-γ and TNF by T cells, leading to the activation of numerous IFN-responsive genes via signal relay and the transcription activator STAT1. However, this model represents only a fraction of the over 1300 genes positively regulated in psoriatic changes. Activated DCs may collaborate with IFN-α, IL-20, IL-12, and IL-23 in an inflammatory cascade. Additionally, other cytokines produced by keratinocytes or stromal cells likely regulate the proliferation and fibrosis of epithelial-stromal (vascular) structures in psoriatic lesions. [15], [16]
Oxidative stress and psoriasis
Oxidative stress is imbalance between reactive oxygen species and antioxidant system. [17] Numerous studies have demonstrated the involvement of reactive oxygen species (ROS) and nitric oxide synthases (NOS) in the pathogenesis of psoriasis. The imbalance in redox status and elevated levels of inducible NOS contribute to the generation of oxidative stress, which can result in various molecular abnormalities. ROS encompass a diverse group of oxygen-containing molecules capable of reacting with other substances, and they can be categorized into radicals, including hydrogen peroxide (HO2•), superoxide (O2• −), hydroxyl (OH•), and peroxyl radicals (RO2•), as well as non-radicals such as ozone (O3), hydrogen peroxide (H2O2), and hypochlorous acid (HOCl)(18).
Nitric oxide synthases (NOS) are enzymes responsible for catalyzing the synthesis of nitric oxide (NO), with three isoforms: endothelial NOS (eNOS), neuronal NOS (nNOS), and inducible NOS (iNOS). In psoriasis, iNOS is excessively synthesized by various cell types, including keratinocytes, compared to healthy skin cells, implicating this isoform in the disease's pathogenesis. Oxidative stress arises when the balance between reactive oxygen species (ROS) and antioxidants tilts in favor of ROS, disrupting redox signaling and regulation, and leading to various molecular abnormalities. Studies demonstrate that oxidative stress induced by varying levels of ROS can result in DNA modifications, lipid peroxidation, and the release of proinflammatory cytokines. As second messengers, ROS influence cellular signaling pathways, particularly proinflammatory signaling pathways, and the expression of numerous genes. The human body possesses mechanisms to counteract oxidative stress factors even before they exert detrimental effects on cells. Skin enzymes such as superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx) play critical roles in the antioxidant defense process. Non-enzymatic antioxidants like vitamins E and C, as well as glutathione (GSH), also contribute significantly to antioxidant defense.
In the pathogenesis of psoriasis, mild oxidative stress holds greater significance than severe oxidative stress. There exists a positive correlation between oxidative stress markers and the psoriasis area and severity index (PASI), while an inverse relationship is observed between antioxidant markers and PASI scores. Factors such as total oxidative stress (TOS), plasma or serum malondialdehyde (MDA) levels, and the release of vascular endothelial growth factor (VEGF) from various cell types play pivotal roles in angiogenesis in psoriasis. Additionally, VEGF may drive leukocyte migration through psoriatic skin, thereby exacerbating the inflammatory process. [18], [19], [20]
Rationale for Exploring Natural Products and Emulgel in Psoriasis Therapy
Emulsion gels have emerged as essential pharmaceutical topical semi-solid dosage forms since the 1980s. These gels, categorized as either water-in-oil (W/O) or oil-in-water (O/W) emulsions, are solidified with the assistance of one or multiple gelling agents, constituting two main components: the emulsion and the gel. The incorporation of a gelling agent into the aqueous phase transforms a conventional emulsion into an emulgel, rendering it thixotropic and enhancing the system's bioavailability. [21]
The emulsion component functions as a controlled release system, where drug particles are entrapped within the internal phase. The dispersed phases within the emulsion serve as reservoirs of the drug, gradually releasing it in a controlled manner through the external phase onto the skin. [22] Meanwhile, the gel component forms a cross-linked network, trapping small drug particles and facilitating their controlled release. Additionally, the mucoadhesive property of the gel extends the contact period of the medication on the skin, further enhancing its effectiveness. While gels offer rapid drug release compared to other semisolid preparations, they face limitations in delivering hydrophobic drugs. [23] To address this challenge, emulgels are developed, allowing even hydrophobic drugs to benefit from the advantageous properties of gels. By incorporating an emulsion into a gel matrix, emulgels function as dual-controlled release systems, mitigating issues like phase separation and creaming commonly associated with emulsions.
Emulgels are simple to prepare and cost-effective to manufacture. Their preparation involves simple steps without requiring specialized equipment, and the materials used are readily available and inexpensive. [24] Emulgels can be formulated in two ways: by blending a gelling agent with an aqueous phase or by introducing a gelling agent as a component of the water phase in the emulsion. This versatility in preparation methods contributes to the widespread adoption and practicality of emulgels in pharmaceutical formulations. [25] Emulgels combine the advantages of both emulsions and gels, making them highly favored by patients. They offer numerous benefits as transdermal formulations, including controlled drug release and convenient administration, which improve patient adherence to treatment. [26] Furthermore, the rheological and sensory properties of emulgels enhance their application to the skin. Emulgels designed for dermatological purposes exhibit several desirable properties. They are thickotropic, non-greasy, easily spreadable, and readily removable. Additionally, they provide emollient effects, do not stain clothing, are water-soluble, biocompatible, transparent, have extended shelf lives, and boast pleasing aesthetics. These systems share similarities with the lipoprotein structure of the skin, enabling them to spread more easily over large areas, such as psoriatic lesions, compared to creams or ointments. [27]
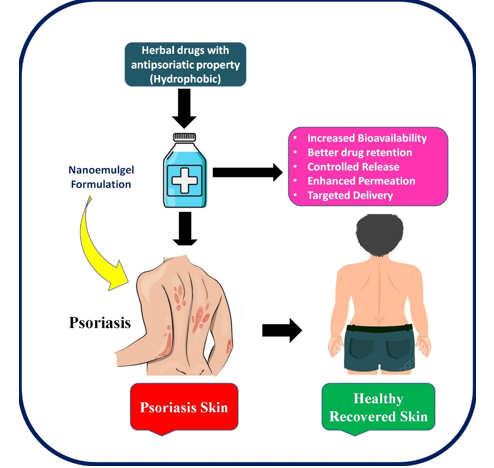
In summary, emulgels have proven effective in treating psoriasis, thanks to their stability, user-friendly application, and compatibility with diverse drug delivery methods. The selection of an ideal consistency of gelling agents is paramount, as it directly impacts the mechanical and sensory characteristics of the formulation, as well as the comfort of use for patients. By carefully considering these factors, emulgels can continue to serve as valuable tools in managing psoriasis effectively. The Diagrammatic representation of applicability of emulgel formulation for phototherapy of Psoriasis shown in.[Figure 1]
Natural Products in Psoriasis Treatment
a) Aloe vera
Aloe vera, a well-known plant with applications in burn treatment and skincare, contains six antiseptic compounds—lupeol, salicylic acid, urea nitrogen, cinnamonic acid, phenols, and sulfur—that individually inhibit the growth of fungus, bacteria, and viruses.[28] Psoriatic plaques were successfully removed in 83.3% of treated patients in a 1995 double-blind, placebo-controlled research involving 60 patients with psoriasis vulgaris when aloe vera extract (0.5%) was added to a hydrophilic cream, as opposed to 6.6% in the placebo group. Aloe vera, a perennial succulent belonging to the Liliaceae family, produces a colorless, mucilaginous gel with various potential pharmacological actions, including anti-inflammatory properties. This gel, used for cosmetic and therapeutic purposes, has been deemed a successful psoriasis treatment without any drug-related adverse effects. [29], [30]
Curcumin
Curcumin, a constituent found in turmeric with a rich history of use in Southeast Asia, has been recognized for centuries for its diverse medicinal properties, including antioxidant, anti-inflammatory, antimicrobial, and anticancer effects. [31], [32] Extensive research has established curcumin as a safe and non-toxic substance for humans, with doses of up to 8 g per day considered well-tolerated. [33] Its potential efficacy in combating psoriasis has been explored, with molecular docking studies revealing its interaction with TNF-α receptor-binding sites. This interaction, involving residues like Leu89, Asn90, Asp105, Asn106, and Cys129, indicates that curcumin directly influences TNF-α, disrupting signal transduction and suppressing inflammation induced by this cytokine. [34]
Clinical trials have demonstrated the tolerability of oral curcumin in psoriasis patients, although conclusive evidence requires extensive, placebo-controlled trials. While overall response rates were modest, promising results in specific individuals suggest further investigation. [35] In vivo studies on mice by Tu et al.indicated that curcumin inhibits TLR2, TLR4, and TLR-9 expression, potentially reducing proinflammatory cytokine levels and enhancing the anti-inflammatory IL-10. This implies that curcumin may be used to treat inflammatory illnesses by acting as an immunomodulatory and anti-inflammatory drug. [36] Curcumin suppresses TNF-induced production of IL-1ß, IL-6, and TNF in TNF-treated HaCaT cells, according to in vitro studies by Cho et al. Curcumin's potential as an immunomodulatory drug is highlighted by the correlation between its inhibitory impact on cytokine production and the reduction of MAPKs and NF-B. Curcumin has been shown by Sun et al. to suppress TNF-induced NF-B activation and the production of IL-6/8 in HaCaT cells, suggesting its role in minimizing keratinocyte-related inflammation through NF-B inhibition. [37]
Additionally, curcumin has demonstrated potential as a phosphorylase kinase activity (PhK) inhibitor. PhK activity is linked to psoriatic activity. Curcumin has the ability to cure psoriasis locally, as evidenced by the reduced PhK levels seen in platelet samples treated with a water-alcohol extract from the rhizome of turmeric.. [38] Curcumin has been shown in vitro to suppress proinflammatory cytokines and keratinocyte proliferation in a variety of cell types, indicating that it may find use in the treatment of hyperproliferative disorders such as psoriasis. Curcumin was discovered to suppress TNF's anti-apoptotic action, hence preventing the progression of psoriasis in HaCaT cells treated with TNF-α. [39]
Genistein
Genistein, a flavonoid commonly found in various vegetables such as soybeans and fava beans, occurs in food at concentrations ranging from 1 to 2 mg/g. Extensive research has elucidated its manifold biological effects, encompassing antioxidant, antiangiogenic, and anticancer properties. [40] In vivo investigations by Wang et al. demonstrated that in a mouse model of psoriasis, administration of genistein at doses of 50 and 100 µM for 2 hours resulted in a reduction in the expression of cytokines such as IL-1β, IL-6, TNF-α, CCL2, IL-17, and IL-23. Furthermore, they observed that genistein inhibited STAT3 phosphorylation, IκB phosphorylation, and nuclear translocation of NF-κB in both IMQ-treated mouse skin and TNF-alpha-stimulated HaCaT cells. [41] In vitro studies conducted by Smolińska et al. revealed that treating HaCaT cells with genistein at a dose of 1 µg/mL for 24 hours suppressed the generation of reactive oxygen species (ROS) when stimulated by TNF-α or LPS. These findings suggest that in the psoriatic model, genistein has the potential to alleviate ROS-mediated NF-κB activation and NF-κB-dependent inflammatory cytokine production, particularly in keratinocytes stimulated by TNF or LPS. [42]
Epigallocatechin-3-gallate (EGCG)
Green tea contains the flavonoid EGCG, whereas black tea contains tannic acid, quercetin, and the flavonoids theaflavin and thearubigin. [43] Anti-inflammatory, anticancer, antioxidant, and anti-ultraviolet radiation activities are among the advantages of EGCG that have been documented. In order to create a model of psoriasis, Zhang et al. used dosages of 0.25 g and 12.5 mg administered over a period of 6 days to IMQ-stimulated mice. [44] According to their research, local EGCG administration decreased PCNA (proliferating cell nuclear antigen) expression, which successfully prevented aberrant epidermal cell proliferation brought on by IMQ and reduced psoriasis symptoms. Moreover, the investigation showed a reduction in SOD and CAT activity following EGCG administration, indicating that EGCG may lessen mouse psoriasis symptoms via controlling antioxidant variables.
|
Sr. No. |
Active Constituent |
Plant Sources |
Mode of Action |
Ref. |
|
1 |
Curcumin |
Curcuma longa L. (Turmeric) |
NFKB is inhibited with a selective phosphorylase kinase inhibitor, which lowers inflammation. |
|
|
2 |
Colchicine |
Colchicum autumale L. (Autumn crocus) |
Antichemotactic. |
|
|
3 |
Artesunate |
Artemisia annua L. (Sweet Wormwood) |
Controlling the expression of CXCR2 and boosting TGF-1 secretions in vitro to have an antiproliferative effect. |
|
|
4 |
Camptothecin |
Camptotheca acuminate Decaisne (Heaven wood tree) |
Limiting proliferation and promoting differentiation. |
|
|
5 |
Podophyllotoxin |
Podophyllum peltatum L. (Mayapple) |
Inhibits the growth of keratinocyte and triggers apoptosis |
|
|
6 |
Iso-Comptothecin |
amptotheca acuminate Decaisne (Heaven wood tree) |
Inhibits the growth of keratinocyte and triggers apoptosis |
|
|
7 |
Hypericine |
Hypericum perforatum L. |
Alleviated erythema, desquamation, and erosions by penetrating the skin with a photoactive concentration |
|
|
8 |
Thymoquinon |
Nigella sativa |
Ethosomal vesicular system could be use as delivery medium to increase drug solubility, trapping, and penetration. |
|
|
9 |
Aloe emodin acemannam, salicyclic acid. |
Aloe barbadensis miller |
intervene with various proinflammatory pathways, such as inhibiting NF-κB, MAPK, and PI3K signaling and reducing iNOS, IL-6, and IL-1β production macrophages, or decreasing levels of prostaglandin E2 via COX blockade |
|
|
10 |
Silymerin, Vitamin E taxifolin, linolenic acid and linoleic acid. |
Silybum marianum |
cAMP phosphodiesterase, enhance hepatic endotoxin clearance, and prevent leukotriene production |
|
|
11 |
Capsaicin |
Capsicum annuum |
inhibit NF-κB and AP-1 signaling, influencing inflammation |
|
Type |
Gelling Agent |
Conce. of Gelling Agent |
Drug |
Key Findings of Effectiveness of Action |
Ref. |
|
Emulsion |
Cremophor EL |
Not specified |
Calcipotriol |
Improved drug release compared to commercial cream |
|
|
Emulsion |
Carbopol 940 |
0.6–1.2% |
Calcipotriol |
Higher release rate compared to commercial ointment |
|
|
Microemulsion |
Carbopol 940 |
1% w/w |
Cyclosporine |
Improved permeation compared to cyclosporine suspension |
|
|
Nanoemulsion |
Pluronic F127 |
1% |
Leflunomide |
Enhanced therapeutic response and reduced systemic side effects |
|
|
Emulsion |
Carbopol 940 |
0.2–1.5 g |
Aqueous coffee extract, Myrrh alcoholic extract, Cymbopogon proximus, Nigella sativa seeds total oil, alcoholic extract, Theophylline |
Promising new herbal formula for psoriasis treatment |
|
|
Nanoemulsion |
Carbopol 934 |
0.25–1.0% w/w |
Curcumin |
Improved permeation and quicker healing compared to commercial gel |
|
|
Nanoemulsion |
Carbopol 971 |
1% |
Betamethasone Dipropionate |
Good stability and in vivo anti-inflammatory activity |
|
|
Microemulsion |
Carbopol 934, Carbopol 940 |
Not specified |
Commiphora mukul Psoralea corylifolia |
Good anti-inflammatory activity |
|
|
O/W Microemulsion |
Carbopol 934 |
3% |
Betamethasone Dipropionate, Salicylic Acid |
Improved spreadability and in vivo anti-inflammatory activity |
Rutin
Rutin, a polyphenolic hydrophobic compound classified within the flavonoid family, is naturally occurring in various foods such as citrus fruits, apples, Betula leaves, buckwheat, black tea, and green tea. Renowned for its participation in antioxidant and anti-inflammatory processes, rutin has garnered attention in experimental research to evaluate its potential as an active ingredient in medicinal products. [63], [64] Derived from Memecylon malabaricum, a small tree distinguished by its blue flowers, rutin's antipsoriatic properties were investigated in in vivo studies employing a mouse tail test, as well as in vitro antipsoriatic activity using HaCaT cells at a concentration of 100 mg/mL. The research findings unveiled robust antipsoriatic activity of the plant in the mouse tail test, although it did not exhibit significant activity in any of the three conducted in vitro tests. Despite the modest activity observed in the LOX inhibition assay, Memecylon malabaricum demonstrated potent in vivo activity. These results underscore the antipsoriatic potential of the entire M. malabaricum leaf, thereby corroborating its traditional use by Siddha healers. [65]
Silybum marianum
Silybum marianum, commonly known as milk thistle, is effective in treating psoriasis due to silymarin's capacity to inhibit cAMP phosphodiesterase, enhance hepatic endotoxin clearance, and prevent leukotriene production. [66] Phytochemicals present in milk thistle, including silymarin, particularly silybin, contribute to its biological functions. [67] Tea tree oil, derived from Melaleuca alternifolia, is renowned for its wound-healing capacity. The essential oil of Melaleuca alternifolia, rich in constituents like terpinen-4-ol, 1,8-cineole, α-terpineol, terpinolene, α- and γ-terpinene, is utilized for medical purposes.[68]
Thespesia populnea
Thespesia populnea, historically used to cure various skin conditions, including psoriasis, involves external application of oil made by boiling powdered bark in coconut oil. [69] However, there is no confirmed scientific data on its anti-psoriatic activity, prompting the selection of Thespesia populnea for scientific evidence establishment. [70] Mahonia aquifolium, also known as Barberry, contains isoquinoline alkaloids such as berberine, making it an anti-inflammatory drug used to treat skin conditions, including psoriasis. [71]
Emulgels in Dermatological Applications
Emulgels represent a crucial drug delivery system, especially for administering hydrophobic active ingredients. They boast properties such as being non-toxic, non-irritating, non-sensitizing, making them highly suitable for various applications. [72] The key to formulating an effective emulgel lies in meticulously selecting the oil phase, emulsifier, and gelling agent. By choosing the appropriate emulgel excipients, optimal release of active ingredients can be achieved, facilitating their permeation through biological barriers such as the skin or intestinal mucosa. Consequently, this enhances their biological or pharmacological effects, ensuring the efficacy of the delivered therapeutic agents. [73]
The controlled release mechanisms inherent in emulgels enable controlled release and targeted drug delivery. These mechanisms arise from the presence of both an emulsion and a gel system within the formulation. Various formulation factors, including the particle size of a colloidal system, surfactants, and polymers serving as gelling agents in emulgels, significantly influence the release and membrane transport of active substances. The particle size of a colloidal system plays a pivotal role in shaping the release profile of substances encapsulated within the particles. Smaller particle sizes facilitate enhanced release and penetration of active substances through the skin. Consequently, careful manipulation of these formulation factors allows for precise control over drug release kinetics and targeted delivery, ensuring optimal therapeutic outcomes. [74], [75], [76]
Gelling agents in emulgels improve the stability of emulsions by boosting the viscosity of the continuous phase, leading to a slower release of active ingredients. Higher drug loading speeds up release rates, along with the inclusion of penetration enhancers in emulgels. Emulgels serve as essential carrier systems, especially for delivering hydrophobic active ingredients. Vesicular lipid systems offer a key advantage by accommodating both hydrophobic and hydrophilic drug molecules within them.
Gelling agents
Gelling agents are incorporated into a suitable medium where they dissolve or disperse, forming a weakly cohesive three-dimensional structural network with a high degree of cross-linking, achieved either physically or chemically. This process results in the production of semisolid systems. These agents are categorized into natural, synthetic, and semi-synthetic based on their origin. Natural gelling agents offer notable biocompatibility and biodegradability, although they are susceptible to microbial degradation. Examples include bio-polysaccharides or their derivatives, as well as proteins. [77], [78] In contrast, emulgel formulations commonly utilize various types of semi-synthetic and synthetic gelling agents. Semi-synthetic gelling agents exhibit superior stability and resistance to environmental influences compared to their natural counterparts. [79]
Emulsion gels often utilize natural gelling agents like soy protein, whey protein, pectin, carrageenan, among others, for delivering functional food ingredients. Soy protein isolate (SPI) emerges as a favorable alternative to animal-based protein owing to its cost-effectiveness, nutritional benefits, and excellent functional attributes. Nonetheless, SPI alone may not yield gels with optimal stability properties, prompting the addition of polysaccharides to enhance gel characteristics. Wheat bran cellulose proves particularly effective in enhancing the gel properties of SPI, facilitating the development of formulations with desirable functional attributes. [9], [10]
In recent times, there has been considerable interest in alginate-based food emulgels, which are created through the ionic cross-linking of alginates with divalent cations, predominantly calcium. Alginates have been combined with both traditional and protein-based emulsifiers in emulgel formulations. The gelation process and the formation of emulsion gel beads are influenced by the concentration of alginate, as well as the concentrations of protein and the oil phase. These factors can consequently impact the encapsulation, stability, and release of the encapsulated hydrophobic active substances.
Conclusion
The therapeutic landscape for psoriasis is evolving, with the development of polymeric emulgels as drug carriers promising to address limitations and meet diverse needs. The complexity of psoriatic lesions necessitates tailored treatment strategies. Emulgels offer versatile platforms for developing novel formulations like emulgels. As psoriasis prevalence increases, further research into polymeric gels is needed to enhance treatment outcomes. Understanding texture and rheological properties can improve treatment effectiveness and patient tolerability. Prioritizing formulations that meet patient preferences can optimize treatment outcomes and improve the quality of life for psoriasis patients.
Source of Funding
None.
Conflict of Interest
None.
References
- Singh N, Sondhi S, Jindal S, Pandit V, Ashawat M. Treatment and management for patients with mild to severe psoriasis: A review. Asian J Pharm Res. 2020;10(4):286-92. [Google Scholar]
- Bochénska K, Smolińska E, Moskot M, Banecka J, Cimińska M. Models in the research process of psoriasis. Int J Mol Sci. 2017;18(12). [Google Scholar]
- Sales R, Torres T. Psoriasis and metabolic syndrome. Acta Dermatovenerologica Croat. 2014;22(3):169-74. [Google Scholar]
- Wain T, Venning V, Consuegra G, Peñas P, Wells J. Management of cutaneous T-cell lymphomas: Established and emergent therapies. Australas J Dermatol. 2019;60(3):200-8. [Google Scholar]
- Flynn G. Cutaneous and transdermal delivery-processes and systems of delivery. Mod Pharm Fourth Ed Revis Expand. 2002. [Google Scholar]
- Buwalda S, Vermonden T, Hennink W. Hydrogels for Therapeutic Delivery: Current Developments and Future Directions. Biomacromolecules. 2017;18(2):316-46. [Google Scholar]
- Qghhq L, Evwudfw K, Frsshuqlfxv Q, Ri L. Emulgel : a New Platform for Topical Drug Delivery. Int J Pharma Bio Sci. 2012;3(1):485-98. [Google Scholar]
- Thomas A, Dapkekar M, Nagore D, Doke R, Bankar N, Surve N. Herbal Emulgel Containing Azadirachta indica (Neem) and Nigella Sativa L. Anc Sci Life. 2024;38:141-50. [Google Scholar]
- Abdullah, Liu L, Javed H, Xiao J. Engineering Emulsion Gels as Functional Colloids Emphasizing Food Applications: A Review. Front Nutr. 2022;9. [Google Scholar]
- Lu Y, Mao L, Hou Z, Miao S, Gao Y. Development of Emulsion Gels for the Delivery of Functional Food Ingredients: from Structure to Functionality. Food Eng Rev. 2019;11(4):245-58. [Google Scholar]
- Light K, Karboune S. Emulsion, hydrogel and emulgel systems and novel applications in cannabinoid delivery: a review. Crit Rev Food Sci Nutr. 2022;62(29):8199-229. [Google Scholar]
- Ogawa E, Sato Y, Minagawa A, Okuyama R. Pathogenesis of psoriasis and development of treatment. J Dermatol. 2018;45(3):264-72. [Google Scholar]
- Boehncke W. Etiology and Pathogenesis of Psoriasis. Rheum Dis Clin North Am. 2015;41(4):665-75. [Google Scholar]
- Tokuyama M, Mabuchi T. New treatment addressing the pathogenesis of psoriasis. Int J Mol Sci. 2020;21(20):1-16. [Google Scholar]
- Kapoor B, Gulati M, Rani P, Gupta R. Psoriasis: Interplay between dysbiosis and host immune system. Autoimmun Rev. 2022;21(11). [Google Scholar] [Crossref]
- Bos J, Ri MD, Teunissen M, Piskin G. Psoriasis: Dysregulation of innate immunity. Br J Dermatol. 2005;152(6):1098-107. [Google Scholar]
- Doke R, Pansare P, Sainani S, Bhalchim V, Rode K, Desai S. The Counteracting Performance of Phytoconstituents Against Neurodegeneration Involved in Parkinson’s Disease. J Sci Res. 2021;65(01):146-58. [Google Scholar]
- Lin X, Huang T. Oxidative stress in psoriasis and potential therapeutic use of antioxidants. Free Radic Res. 2016;50(6):585-95. [Google Scholar]
- Cannavò S, Riso G, Casciaro M, Salvo D, Gangemi E. Oxidative stress involvement in psoriasis: a systematic review. Free Radic Res. 2019;53(8):829-69. [Google Scholar]
- Kadam D, Suryakar A, Ankush R, Kadam C, Deshpande K. Role of oxidative stress in various stages of psoriasis. Indian J Clin Biochem. 2010;25(4):388-92. [Google Scholar]
- Parhi R. Recent Advances in the Development of Semisolid Dosage Forms. . Pharm Drug Prod Dev Process Optim. 2020. [Google Scholar]
- Shivakalyani A, Seeram R. Controlled Drug Delivery Systems: Current Status and Future Directions. Mol [Internet]. 2021;26(19). [Google Scholar]
- Okur N, Bülbül E, Yağcılar A, Siafaka P. Current Status of Mucoadhesive Gel Systems for Buccal Drug Delivery. Curr Pharm Des. 2021;27(17):2015-40. [Google Scholar]
- . Emulgel: An Effective Drug Delivery System. Res J Pharm Technol. 2023;16(6):2754-62. [Google Scholar]
- Hasan S, Bhandari S, Sharma A, Garg P. Emulgel: A Review. Asian J Pharm Res. 2021. [Google Scholar]
- Ahmed S, Verma S, Khan S, Sharma A. Emulgel: A revolution in topical drug delivery system. Int J Health Sci (Qassim). 2022. [Google Scholar]
- Rivero C, López-Gómez J. Unlocking the Potential of Fermentation in Cosmetics: A. Rev Fermentation. 2023;9(5). [Google Scholar]
- Riaz S, Ashraf M. . Recent Advances in Development of Antimicrobial Textiles. 2020. [Google Scholar]
- CC, PB, BS, PS. A prospective, randomized clinical trial comparing topical aloe vera with 0.1% triamcinolone acetonide in mild to moderate plaque psoriasis. J Eur Acad Dermatology Venereol [Internet]. 2010;24(2):168-72. [Google Scholar]
- Verma S. Aloe vera their chemicals composition and applications: A review. Int J Biol Med Res. 2011;2:466-71. [Google Scholar]
- Doke R. Restorative potential of curcumin in Parkinson’s disease. Inven J Mol Pharmacol. 2019;1(2):1-6. [Google Scholar]
- Shehzad A, Wahid F, Lee Y. Curcumin in cancer chemoprevention: Molecular targets, pharmacokinetics, bioavailability, and clinical trials. Arch Pharm. 2010;343(9):489-99. [Google Scholar]
- Kanai M, Yoshimura K, Asada M, Imaizumi A, Suzuki C, Matsumoto S. A phase I/II study of gemcitabine-based chemotherapy plus curcumin for patients with gemcitabine-resistant pancreatic cancer. Cancer Chemother Pharmacol. 2011;68(1):157-64. [Google Scholar]
- Gupta S, Prasad S, Kim J, Patchva S, Webb L, Priyadarsini I. Multitargeting by curcumin as revealed by molecular interaction studies. Nat Prod Rep. 2011;28(12):1937-55. [Google Scholar]
- Kurd S, Smith N, Vanvoorhees A, Troxel A, Badmaev V, Seykora J. Oral curcumin in the treatment of moderate to severe psoriasis vulgaris: A prospective clinical trial. J Am Acad Dermatol. 2008;58(4):625-56. [Google Scholar]
- Tu C, Han B, Yao Q, Zhang Y, Liu H, Zhang S. Curcumin attenuates Concanavalin A-induced liver injury in mice by inhibition of Toll-like receptor (TLR) 2, TLR4 and TLR9 expression. Int Immunopharmacol. 2012;12(1):151-8. [Google Scholar]
- Cho J, Lee K, Kim C. Curcumin attenuates the expression of IL-1β, IL-6, and TNF-α as well as cyclin E in TNF-α-treated HaCaT cells; NF-κB and MAPKs as potential upstream targets. Int J Mol Med. 2007;19(3):469-74. [Google Scholar]
- Heng M, Song M, Harker J, Heng M. Drug-induced suppression of phosphorylase kinase activity correlates with resolution of psoriasis as assessed by clinical, histological and immunohistochemical parameters. Br J Dermatol. 2000;143(5):937-86. [Google Scholar]
- Gupta S, Patchva S, Aggarwal B. Therapeutic roles of curcumin: Lessons learned from clinical trials. AAPS J [Internet]. 2013;15(1):195-218. [Google Scholar]
- Polkowski K, Mazurek A. Biological properties of genistein. Acta Pol Pharm. 2000;57(2):135-55. [Google Scholar]
- Wang A, Wei J, Lu C, Chen H, Zhong X, Lu Y. Genistein suppresses psoriasis-related inflammation through a STAT3-NF-κB-dependent mechanism in keratinocytes. Int Immunopharmacol. 2019;69:270-8. [Google Scholar]
- Smolinska E, Moskot M, Jakóbkiewicz-Banecka J, Wegrzyn G, Banecki B, Szczerkowska-Dobosz A. Molecular action of isoflavone genistein in the human epithelial cell line HaCaT. PLoS One. 2018;13(2). [Google Scholar] [Crossref]
- Mieczan A, Mieczan T, Wójcik G. Importance of redox equilibrium in the pathogenesis of psoriasis-impact of antioxidant-rich diet. Nutrients. 2020;12(6):1-27. [Google Scholar]
- Zhang S, Liu X, Mei L, Wang H, Fang F. Epigallocatechin-3-gallate (EGCG) inhibits imiquimod-induced psoriasis-like inflammation of BALB/c mice. BMC Complement Altern Med. 2016;16(1). [Google Scholar] [Crossref]
- Somboonwong J. Herbal medicine and mechanisms for cutaneous wound healing. Chinese Herbs Herb Med Essent Components. Clin Appl Heal Benefits. 2015. [Google Scholar]
- Dixit N, Baboota S, Kohli K, Ahmad S. Silymarin: A review of pharmacological aspects and bioavailability enhancement approaches. Indian J Pharmacol. 2007;39(4):172-81. [Google Scholar]
- Bernstein J, Parish L, Rapaport M, Rosenbaum M, Roenigk H. Effects of topically applied capsaicin on moderate and severe psoriasis vulgaris. J Am Acad Dermatol. 1986;15(3):504-11. [Google Scholar]
- Wahba A, Cohen H. Therapeutic trials with oral colchicine in psoriasis. Acta Derm Venereol. 1980;60(6):515-35. [Google Scholar]
- Jin H, Zhang R, Gao Y. Effect of Artesunate on Keratinocyte Cultured in Vitro. Chin J Trad Med Sci Tech. 2007;14:176-8. [Google Scholar]
- Lassus A, Rosen B. Response of solitary psoriatic plaques to experimental application of podophyllotoxin. Dermatology. 1986;172(6):319-41. [Google Scholar]
- Kamuhabwa A, Roelandts R, Witte D. Skin photosensitization with topical hypericin in hairless mice. J Photochem Photobiol B Biol. 1999;53(1-3):110-4. [Google Scholar]
- Traub M, Marshall K. Psoriasis - Pathophysiology, conventional, and alternative approaches to treatment. Altern Med Rev. 2007;12(4):319-49. [Google Scholar]
- Xie J, Huang S, Huang H, Deng X, Yue P, Lin J. Advances in the Application of Natural Products and the Novel Drug Delivery Systems for Psoriasis. Front Pharmacol. 2021;12. [Google Scholar]
- Thilagam M, Tamilselvi A, Chandrasekeran B, Rose C. Phytosynthesis of Silver Nanoparticles Using Medicinal and Dye Yielding Plant of Bixa Orellana L. Leaf Extract. J Pharm Sci Innov. 2013;2(4):9-13. [Google Scholar]
- Kaur A, Katiyar S, Kushwah V, Jain S. Nanoemulsion loaded gel for topical co-delivery of clobitasol propionate and calcipotriol in psoriasis. Nanomed Nanotechnol. 2017;13(4):1473-82. [Google Scholar]
- Naga Sravan Kumar Varma V, Maheshwari PV, Navya M, Reddy SC, Shivakumar HG, Gowda D. Calcipotriol delivery into the skin as emulgel for effective permeation. Saudi Pharm J. 2014;22(6):591-600. [Google Scholar]
- Pandey S, Maulvi F, Patel P, Shukla M, Shah K, Gupta A. Cyclosporine laden tailored microemulsion-gel depot for effective treatment of psoriasis: In vitro and in vivo studies. Colloids Surfaces B Biointerfaces. 2020;186. [Google Scholar]
- Pund S, Pawar S, Gangurde S, Divate D. Transcutaneous delivery of leflunomide nanoemulgel: Mechanistic investigation into physicomechanical characteristics, in vitro anti-psoriatic and anti-melanoma activity. Int J Pharm [Internet]. 2015;487(1-2):148-56. [Google Scholar]
- . Kamal Eldin Hussein E. Topical Herbal Emulgel for Psoriasis Treatment.. . . [Google Scholar]
- Algahtani M, Ahmad M, Ahmad J. Nanoemulsion loaded polymeric hydrogel for topical delivery of curcumin in psoriasis. J Drug Deliv Sci Technol. 2020. [Google Scholar]
- Alam M, Ali M, Alam N, Alam M, Anwer T, Imam F. Design and characterization of nanostructure topical gel of betamethasone dipropionate for psoriasis. J Appl Pharm Sci. 2012;2(10):148-58. [Google Scholar]
- Baboota S, Sharma S, Kumar A, Alam M, Sahni J, Ali J. Nanocarrier-based hydrogel of betamethasone dipropionate and salicylic acid for treatment of psoriasis. Int J Pharm Investig. 2011;1(3). [Google Scholar]
- Hosseinzadeh H, Asl M. Review of the protective effects of rutin on the metabolic function as an important dietary flavonoid. J Endocrinol Invest. 2014;37(9):783-91. [Google Scholar]
- Ganeshpurkar A, Saluja A. The Pharmacological Potential of Rutin. . Saudi Pharm J. 2017;25(2):149-64. [Google Scholar]
- Dhanabal S, Muruganantham N, Basavaraj K, Wadhwani A, Shamasundar N. Antipsoriatic activity of extracts and fractions obtained from Memecylon malabaricum leaves. J Pharm Pharmacol. 2012;64(10):1501-10. [Google Scholar]
- Al-Bazaz H, A, Jasim M. Pharmacological and Pharmacognosticl Activity of Silybum marianum. Al Mustansiriyah J Pharm Sci. 2020;20(3):71-81. [Google Scholar]
- Mudit V, Katiyar S. Molecular mechanisms of inhibition of photocarcinogenesis by silymarin, a phytochemical from milk thistle (Silybum marianum L. Gaertn.) (Review). Int J Oncol. 2010;36(5):1053-60. [Google Scholar]
- Parviz G, Kosar M, Demirci F. Tea Tree (Melaleuca alternifolia (Maiden & Betche) Cheel) Oil an important medicinal essential oil. EMU J Pharm Sci. 2022;5(1):57-74. [Google Scholar]
- Vankudothu N, Chekuri R, Lb N. Study of Antipsoriatic activity and Evaluation of E2A Gene Expression for Psoriasis Levels by RT-PCR of Thespesia Populnea L. Methanolic Leaf Extract. Int J Life Sci. 2018;6(1):6-12. [Google Scholar]
- Herman A, Herman A. Topically used herbal products for the treatment of psoriasis - Mechanism of action, drug delivery, clinical studies. Planta Med. 2016;82(17):1447-55. [Google Scholar]
- Gulliver W, Donsky H. A report on three recent clinical trials using Mahonia aquifolium 10% topical cream and a review of the worldwide clinical experience with Mahonia aquifolium for the treatment of plaque psoriasis. Am J Ther. 2005;12(5):398-406. [Google Scholar]
- Phad A, Dilip N, Ganapathy R. Emulgel: A comprehensive review for topical delivery of hydrophobic drugs. Asian J Pharm. 2018;12:382-93. [Google Scholar]
- And P, Evaluations B. Emulgels: a novel topical drug delivery system. J Pak Assoc Dermatol. 2015;26(3):64-75. [Google Scholar]
- Alexander A, Khichariya A, Gupta S, Patel RJ, Giri TK, Tripathi DK. Recent expansions in an emergent novel drug delivery technology: Emulgel. J Control Release. 2013;171(2):122-154. [Google Scholar]
- Mishra S, Singh S, Singh A, Singh A, Sharma D. Emulgels: A Novel Approach for Enhanced Topical Drug Delivery Systems. Adv Nov Formul Drug Deliv. 2023. [Google Scholar]
- Sabalingam S, Malitha A. A review on emerging applications of emulgel as topical drug delivery system. World J Adv Res Rev. 2022;13(1):452-63. [Google Scholar]
- Torres M, Fierro D, Vera A, Palomino B, Magaña K, Bucio H. Hydrogels classification according to the physical or chemical interactions and as stimuli-sensitive materials. Gels. 2021;7(4). [Google Scholar] [Crossref]
- Shah H, Patel M. Insitu Gelling Systems : An Insight. Inven J. 2022;1(2):1-8. [Google Scholar]
- Alves T, Morsink M, Batain F, Chaud M, Almeida T, Fernandes D. Applications of natural, semi-synthetic, and synthetic polymers in cosmetic formulations. Cosmetics. 2020;7(4):1-16. [Google Scholar]
- Abstract
- Introduction
- Pathogenesis of Psoriasis
- Rationale for Exploring Natural Products and Emulgel in Psoriasis Therapy
- Natural Products in Psoriasis Treatment
- a) Aloe vera
- Curcumin
- Genistein
- Epigallocatechin-3-gallate (EGCG)
- Rutin
- Silybum marianum
- Thespesia populnea
- Emulgels in Dermatological Applications
- Conclusion
- Source of Funding
- Conflict of Interest
- References